



This article was medically reviewed by Kate Davies RN, BSc (Hons), FP Cert, Vice President Medical Women’s Health & Longevity at Ultrahuman.
Most period trackers tell you when your period is coming. Ultrahuman’s Cycle and Ovulation Pro (C&O Pro) goes further — it surfaces ten distinct cycle patterns called Cycle Flags™ that can reveal hidden clues about your reproductive health.
Built on 15 years of OvuSense™ research and trained on more than 260,000 real-world cycles, each flag is anchored in peer-reviewed clinical evidence or in OvuSense™’s clinical database.
Standard trackers often miss short luteal phases, slow temperature rises, anovulatory cycles, Fall after Ovulation™ patterns linked to miscarriage and endometriosis, and Fall to Baseline™ patterns that can flag PMOS (polyendocrine metabolic ovarian syndrome)/PCOS (polycystic ovary syndrome) even in women with otherwise regular cycles.
This guide walks through what each flag means, why it matters, and when to bring it to a clinician.
How Cycle Flags™ work
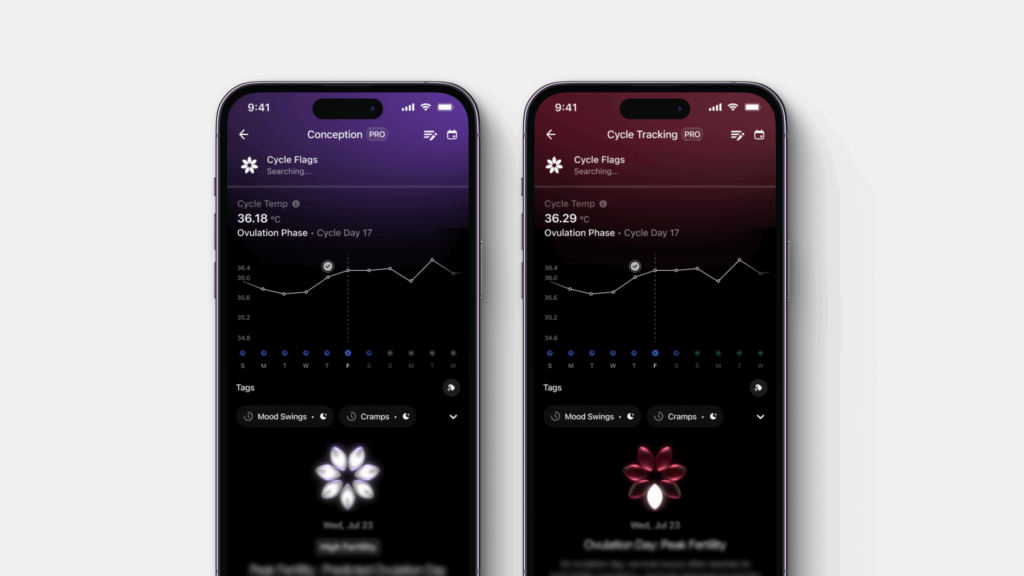
C&O Pro uses your Ring AIR or Ring PRO to track nightly skin temperature across the full cycle. Because skin temperature shifts predictably with progesterone (lower in the follicular phase before ovulation, higher in the luteal phase after), temperature patterns map onto cycle phases with high precision. C&O Pro’s skin-temperature ovulation confirmation has demonstrated over 90% accuracy in the OvuSense™ clinical cohort, identifying both whether ovulation occurred and on which day, based on OvuSense™’s gold-standard algorithm.
Cycle Flags™ layer on top. Each flag is a temperature pattern, defined either by published clinical literature or OvuSense™’s clinical database, that signals something worth understanding. A one off single flag in a cycle is usually nothing to worry about — the signal lives in pattern frequency. A flag that recurs cycle after cycle is what you bring to a clinician, Cycle Report in hand.
Regulatory note — C&O Pro is CE and UKCA certified as a Class IIa medical device in the EU and UK, US FDA registered, and MDSAP certified for Canada and Australia. The cycle-flag detection logic is the same medical-device-grade system used in OvuSense™’s clinical practice.
Why these patterns matter for fertility
Several common reproductive conditions are systematically underdiagnosed because they’re hard to spot from cycle length alone. PMOS/PCOS affects 10-13% of reproductive-age women, with up to 70% of cases undiagnosed (WHO PCOS fact sheet) and goes undiagnosed for years in many. Luteal phase insufficiency (LPI, when progesterone declines too quickly after ovulation) is a common but hard-to-detect contributor to recurrent miscarriage. Anovulatory cycles (where no egg is released) can look like normal cycles because bleeding still happens.
Cycle Flags™ surface these patterns in temperature data, often before symptoms become disruptive. For someone trying to conceive, that shapes whether to keep trying naturally or seek clinical input. For PMOS/PCOS, it refines treatment timing. The menstrual cycle is increasingly recognised as a fifth vital sign — alongside heart rate, blood pressure, respiratory rate, and body temperature — and Cycle Flags™ help build a longitudinal picture of that cycle health.
For context on the temperature physiology underlying these patterns, see Ultrahuman’s luteal phase guide.
Cycle Flags™ explained
Each flag below follows the same structure: what the pattern looks like, why it happens, and when it’s worth acting on.
Three of the 10 flags are proprietary to Ultrahuman + OvuSense™: Fall to Baseline™, False Start™, and Fall after Ovulation™. Research analysing 1,534 cycles from 382 participants (Hurst & Karoshi, Fertility and Sterility 2020) found high odds ratios between these flags and PMOS/PCOS, miscarriage risk, gestational diabetes, and gestational hypertension. An odds ratio greater than 1 means a stronger likelihood the pattern is linked to a given condition — for example, an odds ratio of 2.80 for False Start™ and PMOS/PCOS means women with this flag are significantly more likely to have PCOS than those without.
Think of Cycle Flags™ as a heads-up, not a diagnosis. They’re patterns worth paying attention to, particularly if they appear across multiple cycles, and a useful conversation-starter with a doctor or specialist.
1. Possible Anovulation™
May indicate no ovulation has occurred during the cycle. The biphasic temperature shift — the two-phase pattern that follows ovulation, with the luteal phase temperatures higher than the follicular phase — is absent. Bleeding may still happen, but no egg was released. In OvuSense™’s side-by-side study of 158 cycles in users with known ovulation issues, 23% of cycles were anovulatory (Hurst & Davies, Frontiers in Bioengineering & Biotechnology 2022).
Why it happens: Healthy women experience one to three anovulatory cycles per year without it being a sign of a problem (Hamilton-Fairley & Taylor, BMJ 2003, PMID 12958117). Common causes include being underweight from excessive exercise or restrictive dieting, being overweight, PMOS/PCOS, thyroid disorders, or physical issues with the ovaries.
When it matters: Occasional anovulation is normal. Frequent anovulation — multiple cycles in a row, or several across a six-month window — warrants clinical evaluation. Many causes respond well to treatment, particularly when identified early.
2. Early Ovulation
Ovulation occurs less than 35% of the way through the cycle (Check et al., Clin Exp Obstet Gynecol 2003, PMID 14664409). In a 30-day cycle, that means day 10 or earlier. The follicular phase is shortened.
Why it happens: Early ovulation rises with age and can be triggered by stress, stopping hormonal contraception, or a recent pregnancy. For some women it’s simply their natural pattern. In older women approaching perimenopause, the shortened follicular phase often reflects earlier dominant-follicle selection driven by age-related hormonal changes (Klein et al., J Clin Endocrinol Metab 2002).
When it matters: Early ovulation isn’t inherently linked to infertility, but frequent early ovulation has been associated with a history of recurrent miscarriage (Jukic et al., J Womens Health 2007, PMID 18001191). Worth discussing with a fertility specialist if it’s persistent or you’re trying to conceive.
3. Late Ovulation
Ovulation occurs more than 67% of the way through the cycle. In a 30-day cycle, that means day 21 or later. It can shorten the luteal phase, reducing time available for implantation. Hurst & Citron (OvuSense™, 2020) showed 27% of OvuSense™ users have late ovulation, with a side-by-side study of OvuCore and OvuFirst sensors finding 34% of cycles had late ovulation (Hurst & Davies, Frontiers in Bioengineering 2022).
Why it happens: Occasional late ovulation can happen to anyone. Frequent late ovulation has been linked to PMOS/PCOS and thyroid disorders (both under- and overactive), and can also be influenced by stress, age, or certain medications (Wilcox et al., BMJ 2000, PMID 11082086).
When it matters: Late ovulation by itself isn’t typically a problem. The main concern is when it consistently produces a short luteal phase, which can affect the ability to conceive or sustain a pregnancy. Persistent late ovulation warrants a fertility specialist consultation.
4. Slow Rise™ (Ovulation Detected)
Body temperature rises gradually over several days instead of the typical sharp rise over two to three days. C&O Pro can still detect the biphasic shift within that slow rise, so ovulation is confirmed. Slow rise occurs in an estimated 5% of OvuSense™ users (Gautray et al., Fertil Steril 1981).
Why it happens: Slow rise often reflects a slower progesterone release during ovulation. The ovaries may be having difficulty releasing the egg, or an underlying hormonal imbalance may be affecting the ovulatory process.
When it matters: An occasional slow rise is normal. If it appears frequently and you don’t have a prior PMOS/PCOS or diminished ovarian reserve diagnosis, share with a healthcare provider for evaluation.
5. Slow Rise™ (No Ovulation)
Same gradual-rise pattern, but the rise is so gradual that C&O Pro can’t detect a clear inflection point. Ovulation likely did not occur in the typical way.
Why it happens: Same underlying mechanism as slow rise with ovulation — slower progesterone release. In this version, the rise doesn’t reach the inflection threshold that confirms ovulation.
When it matters: Same guidance — occasional appearance is normal; frequent recurrence warrants clinical evaluation.
6. Short Luteal Phase™
The luteal phase (the time from ovulation to your next period) lasts nine days or less; a healthy luteal phase is typically 11–17 days. OvuSense™ internal data indicates 25% of users have a luteal phase of 10 days or less. A short luteal phase reflects an earlier-than-typical decline in progesterone.
Why it happens: Often triggered by physical or emotional stress, or by conditions that disrupt progesterone stability. When progesterone falls too soon, the body signals the start of the next cycle earlier than expected.
When it matters: A prospective study of 1,635 cycles from 284 women found short luteal phase in 18% of cycles among women with no infertility diagnosis (Crawford & Pritchard, Fertil Steril 2017, PMID 28065408). Many women experience this occasionally. If it appears frequently, consult a healthcare provider about lifestyle factors (stress, over-exercise, nutrition) and possible underlying hormonal conditions. Progesterone support in the luteal phase may be considered when trying to conceive.
7. Long Cycle
A menstrual cycle that lasts more than 45 days from the first day of one period to the start of the next (Grieger & Norman, J Med Internet Res 2020, PMID 32442161).
Why it happens: Most often it points to delayed ovulation occurring later than usual (typically after day 21), or to a cycle where no ovulation occurred at all. Stress, weight changes, excessive exercise, certain medications, and travel can all delay ovulation occasionally.
When it matters: A one-off long cycle is often nothing to worry about. Long cycles that recur should be assessed — they can indicate hormonal imbalance, thyroid disorders, PMOS/PCOS, or hypothalamic amenorrhea (the absence of periods from chronic energy deficit or stress).
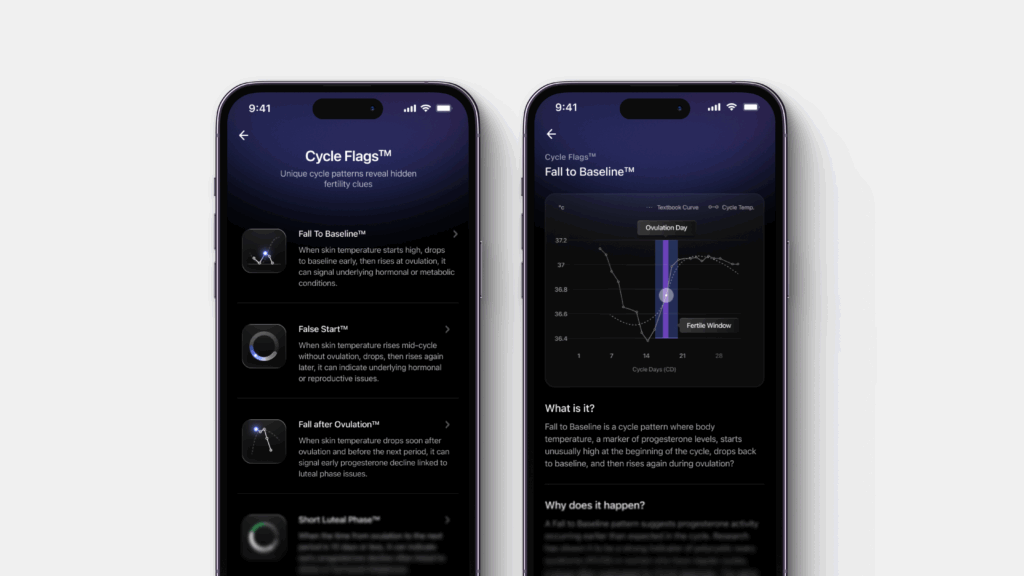
8. Fall to Baseline™
Skin temperature starts unusually high at the beginning of the cycle, drops back to baseline, and then rises again at ovulation. The pattern suggests progesterone activity occurring earlier than expected.
Why it happens: Linked to progesterone activity occurring earlier than expected. First characterised by Hurst & Pirrie (OvuSense™, 2019) and further analysed in Hurst & Karoshi (OvuSense™, 2020), which observed an association between Fall to Baseline™ and PMOS/PCOS in women who otherwise have regular cycles — a population often missed for diagnosis. The same research also observed a link with the later development of gestational diabetes and gestational hypertension.
When it matters: Occasional appearance is normal. Frequent recurrence points to hormonal or metabolic conditions worth evaluation. For anyone already diagnosed with PMOS/PCOS, interpret this flag with a healthcare provider. If it appears before pregnancy, share with your clinician — the association with gestational diabetes and hypertension means earlier monitoring can help. Dietary and lifestyle changes (such as a low-glycemic-index diet) may support cycle normalisation.
9. False Start™
Body temperature rises mid-cycle without ovulation actually occurring, then drops, then rises again later when ovulation does happen. The first rise reflects a brief progesterone surge that doesn’t lead to egg release.
Why it happens: The ovaries begin the process of releasing an egg but don’t succeed at first. Temperature data shows an initial progesterone surge, a drop, and then a stronger second rise when ovulation finally occurs (Baker et al., Temperature (Austin) 2020, PMID 33123618). OvuSense™ clinical research has observed an association between False Start™ and PMOS/PCOS, and a possible link with prior miscarriage history.
When it matters: Occasional appearance is not a problem. Frequent recurrence points to underlying hormonal or reproductive issues worth clinical evaluation, particularly for those already diagnosed with PMOS/PCOS or with a history of miscarriage. Ovarian stimulation (e.g. letrozole) may be considered.
10. Fall after Ovulation™
Body temperature drops rapidly after ovulation, before the next period — progesterone declining earlier than is typical for a healthy luteal phase.
Why it happens: Thought to be linked to luteal phase insufficiency (LPI), when progesterone falls too soon after ovulation, which can affect the ability to sustain a pregnancy. First characterised by Hurst & Pirrie (OvuSense™, 2019). Hurst & Karoshi (OvuSense™, 2020) observed an association between this pattern and miscarriage history; OvuSense™ observational data has also noted a link with endometriosis, though peer-reviewed evidence is still emerging.
When it matters: If this pattern appears in three or more cycles, consult a healthcare provider. Early evaluation matters particularly for those trying to conceive or with a history of reproductive health concerns. Medical treatment and assessment of underlying conditions may help.
How to use Cycle Flags™
Each flag is a pattern indicator, not a diagnosis. The actionable signal comes from frequency. A pattern that appears once and never again is usually not clinically meaningful — a pattern that recurs across multiple cycles is worth bringing to a clinician.
- Track for at least 3-6 cycles before drawing conclusions. This is enough to distinguish one-off variation from a recurring pattern.
- Use the Cycle Report. C&O Pro generates a monthly Cycle Report to share with your healthcare provider. The longitudinal view can speed diagnostic clarity for PMOS/PCOS, thyroid disorders, and luteal phase issues — clinicians often rely on memory and single-cycle bloodwork without it.
- Layer in symptom tracking. Use C&O Pro’s symptom tags (mood, energy, sleep, period flow) to connect how you feel to what’s happening in your cycle phase. Cycle Flags™ + symptom patterns together build a richer picture than either alone.
For broader lifestyle context on how nutrition, movement, sleep, and stress shape hormonal balance, see Ultrahuman’s how to balance hormones naturally guide.
When clinical evaluation still applies
Cycle Flags™ are pattern-detection technology — not a clinical diagnosis. They don’t replace standard PMOS/PCOS, thyroid, fertility, or endometriosis workups. Diagnosis of PMOS/PCOS typically combines cycle history, assessment of symptoms, blood tests for hormone levels, and sometimes an ultrasound.
What they can do is surface patterns earlier, and surface patterns that single-snapshot bloodwork misses. Someone whose Cycle Report shows a Fall to Baseline™ pattern recurring cycle after cycle can bring that pattern data to a clinical conversation, which may speed diagnostic clarity in cases that would otherwise rely on memory and single-cycle bloodwork.
This article is for informational purposes and is not medical advice. Cycle Flags™ are pattern indicators and not a clinical diagnosis. If you have or suspect a reproductive health condition, are trying to conceive, or have other underlying conditions, discuss any findings with your clinician. Disclosure: Ultrahuman sells the Ring AIR and Ring PRO, and Cycle and Ovulation Pro is a fertility-tracking platform built on OvuSense™ technology for complicated cycles, ovulation prediction, and pregnancy planning, with built-in Cycle Flags™ to help users understand cycle patterns and what they mean.



